
Craniosynostoses
Contents
Overview

There are four common types of simple craniosynostosis (cranio = skull, and synostosis = fused bones). Each type of craniosynostosis is caused by a different suture fusing shut. Following a general overview, the four types of synostoses (sagittal, coronal, metopic and lambdoid) are discussed individually, and finally the various ways surgeons treat craniosynostosis are reviewed.
To begin with, it is necessary to first determine if a child actually has craniosynostosis. This is because the most common cause for an abnormal skull shape is not craniosynostosis, but is positional plagiocephaly, caused by outside forces deforming the skull. Positional, or deformational, plagiocephaly is discussed elsewhere on this site (see Deformations).
Skull Growth

To better understand craniosynostosis it is helpful to know a little bit about how the skull grows. The skull is not made up of a single bone but instead is made up of multiple different bones. The junctions where these bones meet are called sutures. We know that the skull does not grow on its own, it only gets larger when the brain is growing. Over the first year or so of life the brain grows very quickly and as it enlarges it stretches the skull bones apart with the sutures acting like expansion joints. We know that when the sutures are stretched by the growing brain this produces chemical signals that tell the skull to add more bone. Should one of these sutures abnormally fuse shut, the skull cannot expand in this area. However, the other non-fused sutures take over and grow more to compensate. This combination of poor growth by a fused suture, and the extra growth that occurs in the remaining open sutures, produces an unusual head shape that eventually becomes obvious to parents, or a pediatrician.
Fusion of the Suture
What causes a suture to fuse shut? The most common reason seems to be pressure on the head while the baby is still in the uterus (womb). We know it is possible to produce craniosynostosis in baby animals by restricting skull growth while growing in the uterus. We also know that the incidence of craniosynostosis is 2 to 3 times higher in twin pregnancies. So, it is very likely that compression plays a primary role in causing craniosynostosis. Children born with a single fused suture may have been positioned in the womb in such a way that there was pressure on a particular region of the head that prevented the skull bones from being stretched apart. If the suture cannot expand it “thinks” its job is done and fuses shut. It is likely that there are genes which, while not directly causing craniosynostosis, do make the sutures stickier or more likely to fuse when compressed. Certain types of craniosynostosis (metopic and sagittal) are more common in boys than girls, leading some researchers to speculate that the male hormone, testosterone, might make craniosynostosis more likely to occur in these sutures. Mothers who have delivered babies with craniosynostosis should not feel guilty they did anything wrong during their pregnancy to cause this. Craniosynostosis occurs despite the mother doing everything right.
When a child born with a single sutural craniosynostosis grows up, it is most likely that they will not pass this trait on to their own children. However, rarely, single sutural synostosis can be passed from generation to generation, suggesting genes may have something to do with this. Some of these genes can be identified with special blood tests. But it should be remembered that most single sutural synostoses appear to be the product of two parents with normal genes, and a mother who has normal prenatal care. For those individuals born with a single sutural synostosis that is not associated with a known gene mutation, the chance of passing on this condition on to their own children is estimated to be around 2-3%. The chance of a couple having a second child with a single sutural synostosis may depend upon which suture was fused. If the metopic suture was involved with their first child, the recurrence risk is about 6%, meaning that were this couple to have 100 more babies, 94 would not be expected to have metopic synostosis. However, if only one coronal suture was involved, this risk falls below 1%. Either way, the chances of another affected child are pretty low.
Finally, there are a few drugs that might be able to contribute to the development of craniosynostosis. Further information can be provided by your surgeon and/or geneticist.
Diagnosing Craniosynostosis
It is important for parents to realize that ridging on their baby’s head does not always mean that a suture is fused. Shortly after birth the sutures are often ridged, until the growing brain flattens them out.
The diagnosis of craniosynostosis is often made following some type of imaging study; the most basic of these is a plain x-ray. On an x-ray, the open sutures appear as dark lines, whereas fused sutures appear as white lines. However, it can sometimes be hard to tell for sure if a suture is open or closed, which is why surgeons more commonly order a CT scan. These scans are the most accurate way to tell if a suture is really closed. Yet, some researchers have raised questions about the long-term effects of radiation associated with these CT scans (which is a lot more than with plain x-rays): specifically, the possibility that this radiation could have a negative effect on intellectual development, or might lead to an increased risk of brain tumors and leukemia (some studies suggest three-fold increases). But these concerns are based on older studies, when CT scans emitted more radiation than today, and it is likely that these scans have become a little safer over time.
However, imaging studies that rely on radiation are usually not necessary for making a diagnosis. It turns out that each different type of craniosynostosis produces a unique head shape. We have published a study showing that a physical examination performed by a craniofacial surgeon is extremely good (98% accuracy) at diagnosing craniosynostosis as compared with CT scans (Publication #28). Therefore, at our center in Dallas, we do not routinely recommend these scans for our patients, reserving this test for those rare cases, where the physical examination is uncertain.
Problems Caused by Sutural Fusion
Studies have shown that over time, pressure can build up inside of the skull in a child with craniosynostosis. This risk seems to be very low in the first 18 months of life but increases as children get older. The problem with pressure building up inside the head is that once it gets high enough, it can reduce blood flow to the brain. The big question every parent wants to know is, can a single sutural synostosis have a negative effect on my child’s development, or intelligence? At present, we believe craniosynostosis either has no significant effect or, if it does, it cannot be measured with current testing. A review of patients treated at our center suggests that the incidence of developmental challenges is no different in our treated patients than is reported for the general population (Publication #101). However, we have seen a much higher frequency and severity of headaches in older children who do develop raised pressure inside their heads, especially if they had been operated on before 11 months of age and have developed a recurrence. We look to future research to be able to better answer the question about the long-term impacts of mild elevations in intracranial pressure.
Does Craniosynostosis Need Treatment?
If one considers all that is known about brain growth and development and then reviews all the studies examining raised intracranial pressure and its effect on blood flow to the brain, it seems clear that most children benefit from an operation to fix their craniosynostosis. Most parents (and some surgeons!) believe the purpose of surgery is to release the restriction by opening up the fused suture. This thinking is incorrect. Surgery cannot create a functioning suture. Once a suture is fused shut, no operation can recreate the growth center. It is lost and gone forever. Instead, the operation needs to accomplish two important things:
- It needs to enlarge the skull enough to improve the blood flow to the brain throughout the child’s entire growth.
- It needs to normalize appearance, so the child looks like everyone else.
When children do not look normal, this can have a profound effect on their personality, their willingness to socially interact with their peers, and even their desire to go to school. The most difficult decision for surgeons and parents comes when children are only mildly affected. When the head shape is only slightly different from normal, it would seem less likely that there could be any significant effects on the brain. In these instances, we may recommend not operating right away and instead suggest following the child conservatively as they grow, reserving surgery only if the shape worsens or if any signs (such as lots of headaches) suggest that pressure might be increasing inside the head.
Listed below are the four major types of single sutural synostoses. For more information on the minor sutural fusions, such as squamosal and low coronal, we recommend discussing these with your surgeon (or you may contact our office).
Listed below are the four types of single sutural synostoses:
Coronal Craniosynostosis (Unilateral Coronal Synostosis, Plagiocephaly)
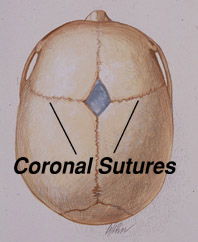

Plagiocephaly is the term used to describe the shape resulting from craniosynostosis involving either the right or left coronal suture. These sutures run across the top of the skull, roughly going from ear to ear. The soft spot, or fontanel, is located at the very top of the skull, halfway between these two sutures. When the coronal suture is fused, the soft spot will usually be closed. On the same side as the sutural fusion, one can often see or feel a raised ridge of bone. When viewed from above, the forehead on the fused side is further back than the opposite side, which has usually slightly overgrown to compensate for the lack of growth on the fused side. In addition, the back of the head will also be flatter on the fused side. In looking directly at the child, the eyebrow will be higher on the fused side, which makes the eye seem more open. Often, parents think that the eye on the other side seems abnormally smaller, when actually it is that the eye on the affected side appears more open because of the closed suture above. Some may notice that their child’s nose is slightly off-center, with the top of the nose angled or pointed towards the side of the fused suture. It is common for parents to say that their child looks worse in a mirror, which may be related to the fact that a mirror flips the image around, so the right side becomes the left; so instead of seeing your child as you are used to, the mirror flips the flatness to the opposite side.
The incidence of plagiocephaly is estimated to be about 1 in 3,500 births, and this occurs more often in girls than in boys. Almost all children affected with plagiocephaly require surgical treatment. A small percentage of children with coronal craniosynostosis will be found when tested, to have a gene mutation indicating a condition called Muenke syndrome. This can be further discussed with your surgeon. The treatment for plagiocephaly is discussed in the Treatment section.
Sagittal Craniosynostosis (Scaphocephaly)
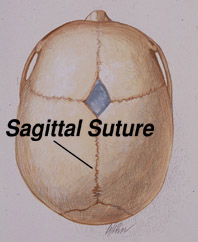

Scaphocephaly is the term used to describe the shape that results from fusion of the sagittal suture. This suture runs from front to back, starting at the fontanel (soft spot) on the top of the head and extending backwards along the midline of the skull. Often, the soft spot will be closed. A ridge can either be seen or felt running along the top of the head. When viewed from above, the skull will be wider closer to the forehead, but gets narrower further towards the back (the opposite of what is normal, where the back of the head is wider than the front). When looking straight on at the child’s face, the forehead may seem bigger, and the sides of the skull look more narrowed. Perhaps the most characteristic finding of sagittal synostosis is that, in looking at your child from the side, the back of the skull is lower than the front, which again, is the opposite of what is normal. The back of the head may also seem to be growing longer. Most children with scaphocephaly will often be found to have a very high head circumference. This is because the skull length must grow abnormally longer to compensate for the reduced width and height of the back part of the skull.
The incidence of scaphocephaly is about 1 in 2,000 births. It is the most common form of craniosynostosis. Almost all children affected with scaphocephaly require surgical treatment. The treatment for this condition is discussed in the Treatment section.
Metopic Craniosynostosis (Trigonocephaly)


Trigonocephaly is the term used to describe the shape that results from craniosynostosis involving the metopic suture. The metopic suture extends from the top of the head at the fontanel, or soft spot, and runs down the middle of the forehead stopping just above the nose. A ridge can usually be seen running down the center of the forehead, and the forehead will appear narrower. The eyes may be spaced closer together than normal. The most characteristic finding is that when looking down from above, the forehead will have a pointed triangular shape like the front of a boat.
The incidence of trigonocephaly is somewhere between 1 in 2,500 and 3,500 births. Trigonocephaly has been reported to occur in mothers who have taken Valproic Acid (Depakene, Depakote, and Convulex) for seizures. Not all children with metopic synostosis require treatment and sometimes it can be very difficult to determine if a child has enough forehead narrowing to require an operation. One reason deciding if surgery is needed can be difficult is, this suture is different from all the other sutures; it is the only one that normally fuses shut in every child, beginning as early as 3 to 4 months of age. Therefore, an x-ray or CT scan showing that this suture has closed is not helpful. It could just be a normal closure. Making this even more difficult is that when this suture normally closes, it can sometimes create a prominent ridge down the center of the forehead without producing the triangular shape, which often worries parents. Children with an isolated ridge running down their foreheads do not require surgery (Publications, Book Chapters #3). Only those children who have actual trigonocephaly need treatment. In Dallas, this decision is made on a physical examination, not by a CT scan, which we believe carries slightly more risk that benefit. The treatment for this condition is discussed in the Treatment section.
Lambdoid Craniosynostosis (Posterior Plagiocephaly)



Posterior plagiocephaly is the term used to describe the head shape caused by craniosynostosis involving one of the two lambdoid sutures. These sutures are located on the back of the skull, one on the right and one on the left, coming together up top like an upside down “V.” When craniosynostosis affects the lambdoid sutures it is usually just on one side. It is extremely rare for both sides to be fused. When viewed from above, the side with the fused suture will be flatter than the opposite side and one can see a low bump (mastoid bulge) behind the ear on the same side as the fused suture. Perhaps the most characteristic sign of lambdoid synostosis is that the height of the skull is lower on the flattened side. Finally, the side of the head across from the affected side will appear to grow outward on this opposite side.
However, the most common cause of a flat back of the head is not craniosynostosis; it is positional plagiocephaly. When there is no reduction in skull height on the affected side, no compensatory bossing on the other side of the skull, and no low mastoid bulge, then a skull deformation, or positional plagiocephaly is most likely. It is critically important to determine whether a child truly has a fused suture because skull deformations do not require surgery. There have been reports in the past of children undergoing unnecessary surgery for presumed lambdoid synostosis that was misdiagnosed by their surgeon, when it turned out all the child had was a deformation. Making the diagnosis even more difficult is that on plain skull x-rays, the lambdoid suture can appear fused when it is actually open. The correct diagnosis of lambdoid synostosis is made either on examination by a highly experienced craniofacial surgeon, or by a CT scan for those with less experience. Children who have lambdoid synostosis do require surgery.
Experienced teams will also look for the development of a Chiari malformation in children with lambdoid synostosis, by getting an MRI scan. A Chiari is when the back part of the brain, called the cerebellar tonsils, pokes down through a hole in the floor of the skull, putting pressure on the spinal cord. We have published a study that revealed over half of children treated for isolated lambdoid synostosis at our center in Dallas were found to have an associated Chiari malformation (Publication #61). When a Chiari is present, this changes the way we recommend treating lambdoid synostosis.
The incidence of lambdoid synostosis is currently unknown but may be as low as around 1 in 50,000 births. One reason for the difficulty in estimating how often this fusion occurs is that it has probably been over-diagnosed in the past. It is certainly one of the least common types of craniosynostosis encountered at craniofacial centers, and therefore this condition is probably best managed at one of the few more highly experienced centers. The treatment for lambdoid synostosis is discussed in the Treatment section.
Other Synostoses
Sometimes, more than one suture can fuse shut. When both coronal sutures are affected, it is more likely that the child might have a syndrome. For a good starting point, please refer to the sections on Apert, Crouzon, and Pfeiffer syndromes. There are also some even more rare conditions in which multiple sutures are fused in different combinations, sometimes referred to as complex craniosynostosis. For more information on this type of craniosynostosis you should either contact your surgeon, or you can contact our office to learn about our research on these rare presentations for craniosynostosis (Publications #27, 41) Once again, these unusual conditions are best treated at the very busiest national centers.
Treatment
Introduction
If surgery is recommended, your child will typically be treated by a craniofacial surgeon and a pediatric neurosurgeon working together as a team. If you meet a neurosurgeon who suggests operating alone without involving a craniofacial surgeon, or vice versa, we recommend seeking a second opinion at another center.
While an experienced pediatric neurosurgeon is essential for the surgical repair, craniofacial surgeons possess the greatest expertise in treating craniosynostosis. During surgery, the craniofacial surgeon decides which parts of the skull should be removed. The neurosurgeon then safely removes these bones, after which the craniofacial surgeon reconstructs the skull.
How is a fused suture reopened? It is a common misconception that all a surgeon needs to do is release the fused suture so that the brain can grow normally afterwards. This is not possible. If a surgeon says they are going to “release” or “open” the fused suture, this should be a sign to consider another opinion. Unfortunately, once a suture has fused shut it cannot be reopened. Advances in our understanding of suture biology have shown that once these growth centers have closed, they can never grow again. Fortunately, during the first 18-months of life, the other sutures take over for the fused suture, preventing increases in intracranial pressure. The skull can also grow another way, by adding layers of bone on the outside and dissolving bone on the inside. Parents are often given the false impression that surgery must be performed quickly to release the fused suture so the brain can grow normally. This is not true. Once fused, there is no way to make a suture grow again. In fact, many studies (including some from our center) show that surgery hurts future skull growth. The earlier the surgery is performed, the worse the skull tends to grow afterwards. It seems the earlier operations are performed, the more likely that a child will need a second operation later in life (Publication #94). For this reason, craniofacial surgeons must carefully balance how long it is safe to delay surgery. The longer you can wait, the better the long-term result, and the lower the chance a second operation might be needed later in life. Doing the wrong operation, lacking experience, and choosing the wrong time to perform the operation, all increase the risk a child will need a second, or even third, operation.
There are many ways your surgeon might recommend treating your child’s craniosynostosis. Below is a brief overview of some of the more commonly performed operations.
*** If a surgeon tells you that your child is nearing a deadline for undergoing a strip craniectomy to prevent potential cognitive impairments or brain damage, we encourage you to immediately seek a second opinion. At present, there is no substantial evidence that earlier surgery provides preventive cognitive benefits. In addition, surgery performed before 11 months of age may carry a greater likelihood of risks than benefits. ***
Older Treatments
The earliest treatments for single sutural synostoses were strip craniectomies (one variation is called the Pi procedure). In this operation a neurosurgeon simply cuts out the fused suture and throws it away. However, studies found that these operations were not as effective as hoped. Depending upon the age of the child, sometimes the removed sections of bone would quickly grow back resulting in a minimal improvement. While in older infants the opposite occurred and the skull never grew back, leaving permanent open spaces of unprotected brain that later needed surgery to repair. From these studies we learned that strip craniectomies seldom normalize the skull shape and are more likely to require a second corrective operation later on. More recent updates on the traditional strip craniectomy procedures (i.e. endoscopic, springs or distraction devices) are described in more detail below.
Recognizing that strip craniectomies alone cannot adequately correct abnormal skull morphology, craniofacial surgeons shifted toward procedures that enlarge and reshape the skull rather than simply excising the fused suture. There are several remodeling strategies, and it is important to ask your surgeon which approach they prefer. For example, in sagittal craniosynostosis, surgeons may choose one of three methods:
- Posterior two-thirds remodeling – surgery is limited to the back portion of the skull surrounding the fused suture (our preferred approach, see The Dallas Procedure below).
- Total cranial remodeling – the entire skull is removed and reshaped, though this larger operation carries slightly higher complication risks and, in our experience, produces less favorable long-term results.
- Staged anterior and posterior remodeling – two separate operations, first addressing the back and later the front of the skull. We believe this unnecessarily doubles surgical risk when the problem can be corrected in a single procedure.
Endoscopic or “Minimally Invasive” Procedures
Some surgical teams have gone back to performing the more traditional strip craniectomy procedure, but now they are changing it up a little. One variation is to use an endoscope. This is basically a small tube through which the surgeon looks to take part of the skull off the dura, or covering of the brain. These operations are frequently done by neurosurgeons working alone, since all that is being done is just removing bone, so there is not much need for a craniofacial surgeon.
The biggest advantages of this technique seem to be that the operation is done through two smaller incisions on the scalp instead of one longer one, and because only a strip of skull is removed, this operation takes less time. But there are also disadvantages. The first is the surgeon can only see by looking down a tube, which limits the view. If there is an accidental injury to the covering of the brain, or bleeding starts up, these complications could be missed. This operation also doesn’t change the shape of the head to make it look more normal. Perhaps most importantly, this operation doesn’t increase the size of the head by very much.
Recognizing that babies do not look very different after the surgery, surgeons often recommend trying to fix the shape by using a helmet, which must be worn 23 hours a day for up to a year after the operation. During this time the family must keep going back to visit a helmet technician, not the surgeon, who adjusts the helmet to force the growing brain to change the shape of the head. This is the opposite of what makes sense to us. The purpose of craniosynostosis surgery is to increase the space inside the head to prevent elevated pressure, not to restrict it.
The term “minimally invasive” is often used by surgeons to describe this operation. Yet, when you think about it, taking part of the protective skull off the brain of a baby is not what most normal people would call a “minimally invasive.” This is a seems to be nothing more than a marketing term that deceptively implies to worried parents that this is a minor operation, and is completely safe. While this operation is shorter because it does a lot less, there is no data showing that using an endoscope reduces the risks of death during this type of craniosynostosis correction compared with an open remodeling procedure.
In our opinion, the most troubling thing about putting a helmet on any baby is that it only changes the shape of the head by restricting growth. Helmets must limit growth the ability of the head to grow across large areas, in order to force the expanding brain to push out the skull bones and change the shape. Once again, this is the exact opposite of what makes sense. We worry that a baby with craniosynostosis might develop pressure inside of the head because the skull cannot grow fast enough. The focus needs to be on enlarging the head; not restricting growth just to improve appearance when the surgeon was unable to do this with their operation.
We believe putting a helmet on a baby that limits growth is sort of like causing craniosynostosis. Our treatment philosophy is to never limit the growth of the head in a baby with craniosynostosis, or any other condition. When remodeling operations are done correctly, the skull is enlarged and the shape is made normal. There is no need for a helmet. This is why at our center we do not recommend endoscopic surgery. We also no longer put helmets on babies for any other reason.
In summary, endoscopic strip craniectomies have:
Advantages:
- Shorter scalp incisions.
- Shorter operation (about 30 minutes shorter operating time than a Dallas Remodeling procedure).
Disadvantages:
- These procedures are not any safer, but carry the concern that complications could be missed from the limited view the surgeon has by having to look through a tube during the operation.
- The operation does not fix the abnormal head shape. Therefore, infants must wear a helmet for up to a year afterwards. It is the helmet therapist who determines the shape of your child’s head, not your surgeon.
- Helmets function like craniosynostosis, they both restrict growth. Any time spent in a helmet must theoretically increase intracranial pressure, to work.
- Part of the skull is thrown away during the operation. If this gap does not completely fill in on its own, a second operation might be later needed to fix the skull to protect the brain.
- These operations must be done early in life because after 14 weeks of age, any missing parts of the skull after surgery will not regrow. But, operating at this early of an age results in worse long-term skull growth, increasing the risks of a second operation many years for raised intracranial pressure.
- This technique cannot over-correct the size of the skull, which is necessary to help prevent the need for another operation 5 to 10 years later.
Spring and Distraction Cranioplasties
Another variation on the traditional strip craniectomy technique involves placing metal springs into the skull (some surgeons prefer metal distraction plates). Currently, only a few surgeons in the U.S. are using these. The way this is done is that, after the surgeon cuts out part of skull, springs or distraction plates are placed across the gap to widen that part of the head. When springs are put it, nothing more needs to be done by the parents. However, when distraction plates are used, parents will notice metal screws poking out through the scalp. They are then instructed to turn these screws every day until their surgeon tells them to stop. For either technique, a second operation is required a couple months later to remove the springs or distraction plates.
Let’s examine the advantages and disadvantages of this method.
Advantages:
- The first operation to remove part of the skull and place the springs or distraction plates is shorter than with a remodeling procedure.
- Springs or distraction plates widen the skull, making the inside of the head larger.
Disadvantages:
- This method requires two operations instead of one. At our Center, we can get the same amount of enlargement with just one operation.
- Two operations double the risk of anesthesia. Some studies raise questions about how anesthesia might affect mental development in infants.
- With springs, there is no way to be exactly sure how much they will widen the head. This depends on many factors: how much skull is removed, how thick and rigid the skull is, the strength of the spring, and how much tension is placed on it. It becomes a bit of a guessing game.
- Springs and distraction plates can only widen in one direction, yet they are used to treat a three-dimensional problem. This makes it unlikely that the head will ever achieve a normal shape afterwards.
- This technique removes part of the skull and then stretches it further. If the resulting hole in the skull doesn’t fill in, another operation may be needed to patch it and protect the brain.
- Studies show that distraction plates carry a complication rate of at least 30%, meaning almost one in three children may suffer some problem. This complication rate is likely even higher for surgeons with less experience.
The Dallas Remodeling Procedure
At our center, surgery to correct craniosynostosis is always performed with both a craniofacial surgeon and a pediatric neurosurgeon working together over the entire operation. We believe having two experienced surgeons working side-by-side improves the speed and safety of the procedure. In addition, only pediatric anesthesiologists with extensive craniofacial surgical experience are selected. Having a highly experienced team not only delivers better results, it also helps prevent serious complications.
Our Center has a special interest in treating craniosynostosis, and we have finely tuned specific treatment protocols for each type. As a result, compared to any other center’s published data, our operative times are shorter and our patients spend less time in the hospital. For example, a typical correction takes under two hours, with a total anesthesia time of just over three and a half hours. Surgery is performed though an incision that runs across the top of the scalp from ear to ear. This wavy “zigzag” incision was developed in Dallas by Dr. Fearon, to improve upon the standard straight-line incision (Publication #10). Making it wavy keeps the scar less noticeable when children get their hair wet. More recently we have shortened the length of this incision, keeping it about inch above each ear, to make the scar even less noticeable. We also do not shave all the hair off for surgery, as many centers routinely do.
The ideal craniosynostosis repair needs to accomplish two things: it must enlarge the inside of the skull, and make the head look more normal. Studies performed at our Center have shown that head growth is reduced after craniosynostosis surgery, with a tendency for the skull to grow back towards its original shape (Publications #26, 32). Based on our research, we now recommend safely delaying surgery longer than has been traditionally done, until somewhere between 11 and 15-months of age. We have also learned that achieving a slight over-correction during surgery reduces the chance that future operations might be needed.
Remodeling operations involve removing and rebuilding parts of the skull. In doing so, it is necessary to hold the bones together while they heal. Although most surgeons use dissolving plates and screws, for many reasons we prefer to use dissolving sutures. We discovered that when surgeons used metal plates and screws to put together the skull, these usually ended up on the inside of the skull as the baby grew, with the screws occasionally poking into the brain (Publication #12). Others have noted this same issue can occur with dissolving plates and screws. While we are unaware of any cases in which this has caused a major problem, many years ago we decided it was safer to use only dissolving stitches to hold the bones together (Publication #20). We have also seen when other surgeons use dissolving plates and screws in children who later come to us for a secondary correction, these plates are sometimes completely covered with bone. Once inside bone, this part of the skull seems less sturdy. For children needing more than one operation, these weakened areas make subsequent skull surgery more difficult. Finally, dissolving plates and screws can sometimes melt into a liquid that eventually drains out through the skin. So, while reconstructing the skull using only dissolving sutures requires a skill that not all surgeons possess, this is what I would want for my own child.
How the repair is done depends upon which suture is fused. The techniques we use today differ significantly from those used many years ago. We follow patients into their teenage years, until their growth is complete, and as a result we have learned a great deal. One of our discoveries is that when surgery is performed on the forehead, the bones can later grow in a lumpy, uneven way. The seams where the bone pieces were joined can also become noticeable many years later, and the forehead may not look normal. Seeing this prompted us to completely change the way we treat the forehead in coronal and metopic synostosis. We believe this newer technique results in better long-term appearance, looks more natural, and lowers chance that a second operation will be needed many years later (our redo operation rate for craniosynostosis appears to be the lowest published). With this newer technique, a single piece of bone (a single-segment reconstruction) is used to rebuild the entire forehead, helping ensure a more natural appearance as children finish growing (Publications #77, #101). For sagittal synostosis, our technique normalizes the appearance of the skull, while also increasing the space inside (Publication #102).
Another unique aspect of the Dallas procedure is when the operation is over, there are no empty spaces left in the skull that could leave the brain unprotected. With strip craniectomies (i.e. endoscopic, springs, or distraction devices) part of the skull is removed with the hope that the body will later fill it back in. Unlike strip craniectomies, remodeling procedures do not throw away any bone, but they do create spaces in the skull as it is enlarged. With the Dallas Procedure, all these gaps are filled using the child’s own bone, so the brain is completely protected afterward. Harvesting the extra bone in babies is not easy, and many surgeons do not seem to consider it important. It also requires a specialized skill that many surgeons may have never learned. This may be why some surgeons do not enlarge the skull during their operations (accomplishing little) or do not take the time to fill in all the open spaces. We believe it is important to ensure the skull is completely rebuilt and intact, without any holes left behind. This may reduce the chance a second operation will later be needed to fill in missing skull areas and even lower the risk for a future brain injury.
When the operation is over, we close with dissolving stitches. We never use metal staples or remove sutures, as these can be painful. We also do not wrap the head with tight bandages or use any drainage tubes, which hurt when removed. While bandages are not “wrong,” they are unnecessary, and drainage tubes probably cause more harm than good. Instead, when finished we simply shampoo the hair and comb it over. It is reasonable to wonder whether a surgeon who still wraps the head with bandages, as was done many years ago, may also be performing an older, more traditional operation.
Our patients typically spend just two nights total in the hospital. The first night is in the pediatric intensive care unit, the safest place to recover. While most children might be ready to leave the hospital 24 hours after their operation, we recommend staying one additional night. The risks of the surgery are very small at more experienced centers. In a published study (Publication #15), we reported the lowest infection rate following craniosynostosis repairs. We also found no infections in babies undergoing first-time operations for craniosynostosis (although this is still possible). A more recent review revealed an overall complication rate of less than 1% out of over 900 craniosynostosis corrections performed by Dr. Fearon (Publication #101).
Older children often tell us after this surgery that they do not have significant pain, although many say their heads feels “tight,” especially at the peak of swelling about 48 hours after the operation. We recommend playing soft music in babies’ rooms after surgery, based on a study showing that music relaxes children and reduces anxiety (and also reduces the amount of pain medicine required). We no longer give children opioids or narcotics after surgery. We have found that giving children a variation of Tylenol and ibuprofen intravenously, instead of by mouth, significantly reduces the risk of postoperative nausea and vomiting (Publication #58) and keeps children very comfortable. Not using any narcotics makes children feel better and go home sooner. This method is called ERAS, or enhanced recovery after surgery. At the most experienced centers, craniosynostosis corrections can be performed at any age, even adults.
Let’s examine the advantages and disadvantages of the Dallas technique.
Advantages:
- With just one operation, the head is enlarged to improve blood flow to the brain, and the overall shape is corrected to look normal.
- We have the shortest published surgical times for any center performing these procedures.
- We also have the shortest length of hospital stay among centers performing remodeling procedures.
- No hair is shaved, no metal staples are placed in the scalp, no drainage tubes are inserted, no head-wrap bandages are used, and we do not give children any narcotics after surgery.
- We believe that we have the best published safety record, and the lowest complication rate (0.7%).
- Although blood loss is slightly higher with remodeling procedures compared to strip craniectomies, we currently have the lowest blood transfusion rate (<3%), even lower than what has been reported with endoscopic repairs.
- We have the lowest published rate of long‑term secondary revisional skull surgeries.
- We strive for personalized “family-doctor-type” care.
Disadvantages:
- Families need to travel to Dallas. Receiving a diagnosis of craniosynostosis and preparing for surgery is already stressful, and travel may add to that stress. (Ninety percent of Dr. Fearon’s patients travel from outside Dallas for treatment, and we have found it is perfectly safe for a child to fly or drive home after surgery.)
- The scalp incisions used are slightly longer than those used in endoscopic repairs, although they are shorter than those used by most surgeons performing remodeling procedures.
When is the best time to do the operation?
Surgery to correct craniosynostosis may be performed at any age, including adults. Below are some of the pros and cons of earlier vs. late surgery.
In favor of an earlier correction are a number of factors:
- With early operations the skull is less rigid and easier to shape.
- The younger the infant, the better the chance that any skull defects left at the end of the operation will later fill in with new bone. This is because somewhere between 4 and 6-months of age, babies pretty much lose their ability to make new skull bone. Therefore, when operating on an older child a few extra steps are necessary in order to fill in all open areas.
- The longer a child grows with a fused suture the more that the unaffected areas of the skull may over-expand in order to compensate, which further changes the skull shape in an abnormal way. A study done at our center suggested that for children born with trigonocephaly, surgery before six months of age might permit slightly better growth between the eyes, an area abnormally narrowed by the fused metopic suture (see Publications #14).
Factors in favor of operating at an older age:
- The operation may be safer. The most serious possible complication following any type of craniosynostosis surgery, whether endoscopic or remodeling, is the child not surviving the operation. We published a two-center review and national Internet survey, examining the likelihood of serious complications during any type of craniosynostosis repair (Publication #37). Our study showed that the most common reason other centers gave for a baby not waking after skull surgery (a complication that is extremely rare and has never occurred with our team in Dallas) is excessive blood loss. Because of this, our Center places a major emphasis on reducing blood loss during surgery. We also recycle blood lost during surgery and return it back to the child before leaving the operating room. As infants grow, their total blood volume increases, which may reduce the likelihood of needing a blood transfusion and may further improve surgical safety. We routinely recommend that infants receive erythropoietin (see Procrit Information) along with iron supplementation before surgery. This medication raises blood levels prior to the operation. We have published research showing that erythropoietin helps prevent the need for blood transfusions, which we believe improves overall safety (Publications #20, #44). In addition, our team routinely uses a “cell-saver,” a machine that recycles blood lost during an operation and washes it, so we can return it to the child before they wake up (Publication #23). These techniques, and many others, make blood transfusions very uncommon at our center (under 5%). One other reason to avoid blood transfusions is that some research suggests that patients who receive them have a higher risk of a postoperative infection.
- Anesthesia may be safer at an older age. Animal studies suggest that during the period of rapid early brain growth, anesthesia might have harmful effects on the brain (http://www.smartttots.org). It is unclear at what age anesthesia becomes completely safe, but it is likely that older is better. Additionally, the fewer times a child undergoes anesthesia, the lower the risks of developmental effects.
- The most significant advantages of operating at an older age is that the results are most likely to last a lifetime. Research from our center, examining long-term skull growth of the skull after craniosynostosis corrections (Publication # 26) showed that the skull does not grow normally after surgery and tends to grow back towards its original shape. Based on this research, we now slightly over-correct the skull shape to reduce the chance that a second operation will be needed. Just as importantly, we have been performing craniosynostosis repairs at an older age than most other centers. Another study we published, which measured growth after surgery for all different types of single-suture craniosynostosis (Publication #32) revealed that the earlier the surgery was performed, the worse the subsequent growth. Poorer growth increases the likelihood another operation may be required many years later. We believe that waiting until children are slightly older, and performing slight over corrections, is the reason why so few of our patients have needed secondary operations compared with other centers large enough to publish their outcomes.
Balancing all these factors, the ideal time to safely correct single sutural craniosynostosis appears to be between 11 and 15-months of age, depending on which suture is involved, the severity of the skull shape abnormality, and several other considerations.
Final Thoughts
It is important to discuss the specifics of any proposed operation with your local surgeon. Make sure you fully understand what is being recommended. Do not hesitate to ask how your child’s operation will be performed and why your surgeon prefers their particular technique. For suggestions on some questions to ask, click on “Choosing a Doctor.” Should you decide that you want the most experienced and specialized care for your child, you can learn more by clicking on “About our Center.”






Examples of a plagiocephaly (left), trigonocephaly (middle) and scaphocephaly (right) seen before surgery (above) and after (below).
Jeffrey Fearon, MD, FACS, FAAP
Director, The Craniofacial Center
7777 Forest Lane, Suite C-700
Dallas, Texas U.S.A.
972-566-6464
cranio700@thecraniofacialcenter.com
*** For those who wish to contact Dr. Fearon by e-mail, it is recommended that you add his e-mail address to your address book. Sometimes e-mail spam filters may block his response to you and there is no way for him to know that you never received his answer. If you send e-mail and do not get a response, please re-send your e-mail after adding cranio700@thecraniofacialcenter.com to your address book, or call us by phone.